


By Erin Sparnon, MEng CSSBB AAMIF and Jeannine Blake, Ph.D., RN
It’s 8:15 a.m. on a Monday when the phone rings again. After nursing rounds, you’re told that four more infusions ran slow over the weekend. The nurses had to scramble to catch up dosing and documentation, and the “problem pumps” are waiting for you in a storage closet – each tagged for testing.
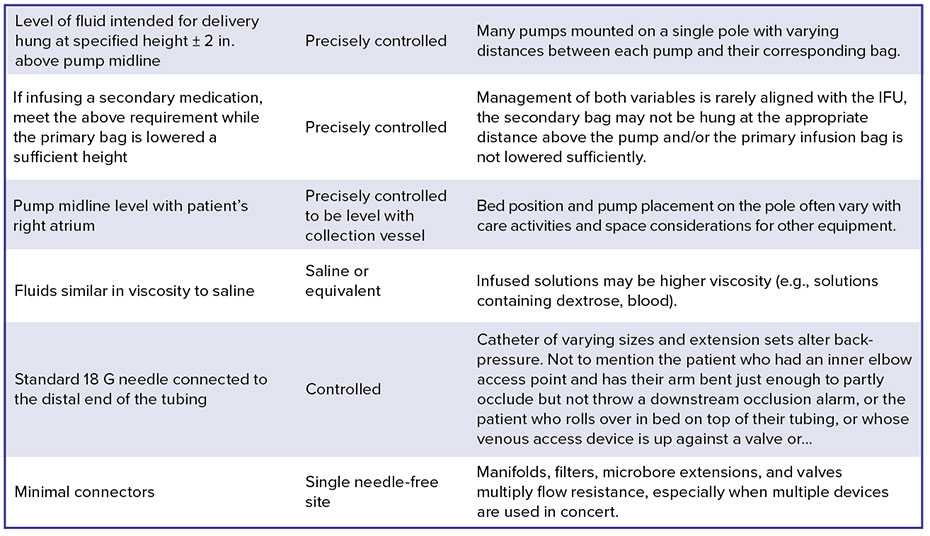
When you bring them to the bench though, every pump checks out perfectly within specifications. It’s the same pattern that’s been playing out for weeks: repeated reports of under-infusion, but no reproducible failures under controlled test conditions. The frustration is understandable, yet also predictable. The Instructions for Use (IFU) for the most common linear peristaltic infusion pumps specify setup conditions that are rarely achievable at the bedside.1,2 This can be due to both physical limitations (e.g., small bed spaces or lack of IV poles) and/or workflow constraints (e.g., understaffing, high-acuity multi-patient assignments). Running your infusion pumps in less-than-ideal conditions can result in clinically meaningful flow-rate inaccuracy, even though the device itself may be functioning (and testing) exactly as designed with ±5 % accuracy.3,4 What does this look like in the wild?
COMMON IFU REQUIREMENTS VS. BEDSIDE REALITY
INVESTIGATING BEFORE YOU TEST
Before launching into calibration checks, ask how the pump was actually used.
Medication & Delivery Context
• What medication or fluid was running? (Viscosity matters.)
• Programmed flow rate?
• Primary or secondary setup?
• Was the bag pharmacy-prepared (no overfill, unless your pharmacy starts overfilling to account for priming volume) or was it a premix/admixture (which could see a possible 5–10% overfill once mixed)?
• If you know the bags are likely to exhibit overfill, is the completion delay consistent with expected overfill?
Access & Setup Factors
• What was the venous access type (central vs. peripheral, and what site) and gauge/French size?
• Pump height relative to patient’s right atrium.
• Use of manifolds, filters, antisiphon valves, or microbore tubing
• Any tubing extensions or atypical accessories
If staff can’t retrospectively answer these questions, consider developing a simple intake checklist for pumps returned for evaluation. Many clinicians are unaware that these factors materially affect flow performance5 and therefore will not always know proactively that this information should be included in an incident report.
WHY THIS MATTERS
Investigating infusion-accuracy complaints means more than proving a pump “passes.” It requires understanding why under-delivery occurred in the clinical context. IFU-based bench testing often bears little resemblance to real-world conditions. Without bridging that gap, we risk undermining trust: when nurses see an infusion run slow but are told the pump is “fine,” it can perpetuate under-reporting, mistrust and frustration on both sides.
WHAT CAN HTM DO ABOUT IT
Let’s expand our concept of customer service and solve the right problem. While it’s tempting to jump immediately into a performance test, we’re helping our nursing colleagues get their jobs done, building trust, and delivering much better overall support if we first pause and take a wider view of the situation. An under-delivering pump isn’t always (or even usually) a broken pump, but instead a symptom of larger challenges that are taking your nursing colleagues away from clinical care. And *that* is an incredibly useful challenge to solve.
While we’ve focused on sources of under-delivery in this article, consider just how many commonly reported pump situations might hint at larger systemic problems:
• Suspected under- or over-delivery
• Too many air in line alarms
• Too many high-pressure/occlusion alarms
Get interested in how these reports might be signaling larger systemic issues, it’s helpful to reframe the question from “is the pump broken?” (or worse, “why do my nurses keep sending me no-fault-found pumps?”) to “what could be going on here?” Get curious, go up on the floors, develop rapport with the nurses, ask how often these problems are being observed and not reported, sit in on nursing rounds … generally see what you can find. This curious mindset will help clinical engineers and HTM professionals turn repeated “no-fault-found” events into meaningful safety learning.
Opinions of the authors are their own.


References
1. Alaris B. BD AlarisTM System with GuardrailsTM Suite MX User Manual. Product Image. 2023:1-684. Accessed February 19, 2019. https://www.bd.com/en-us/offerings/brands/alaris
2. Baxter. Operators Manual Spectrum IQ Infusion System. 2018:1-341. Accessed February 19, 2019. http://pacificmedicalsupply.com/sigma-spectrum-infusion-pump/
3. Blake JW, Meade K, Giuliano KK. Intravenous Smart Pumps: A Review of the Safety Implications for the Most Ubiquitous Technology in US Acute Care. Critical Care Nurse Clinics. 2025:1-21. doi:10.1016/j.cnc.2025.01.004
4. Blake JWC. Intravenous Pump Flow Accuracy: A Systematic Review. J Infus Nurs. Jan-Feb 01 2025;48(1):44-52. doi:10.107/NAN.0000000000000576
5. Giuliano KK, Blake JW. Nurse and Pharmacist Knowledge of Intravenous Smart Pump System Setup Requirements. Biomedical Instrumentation & Technology. 2021;
