
In healthcare, equipment disposition is no longer a back-of-house task relegated to storage rooms and loading docks. It is a decision that must consider clinical operations, cybersecurity, compliance, sustainability and capital recovery. As hospitals and health systems face mounting financial pressures and increasingly complex regulatory requirements, the way they retire, redeploy, resell, recycle or dispose of devices has direct implications for patient safety and the bottom line. In this month’s Roundtable, industry leaders share equipment disposition and recycling insights.
Participants for this discussion are:
- HERO Business Inc. President Kevin Lynskey;
- Image One Medical Group LLC CEO Ric Arcadi; and
- Project C.U.R.E. Director of National Procurement Janet Thomason.
Q: WHAT MISTAKES DO ORGANIZATIONS MOST COMMONLY MAKE WHEN RETIRING MEDICAL EQUIPMENT?
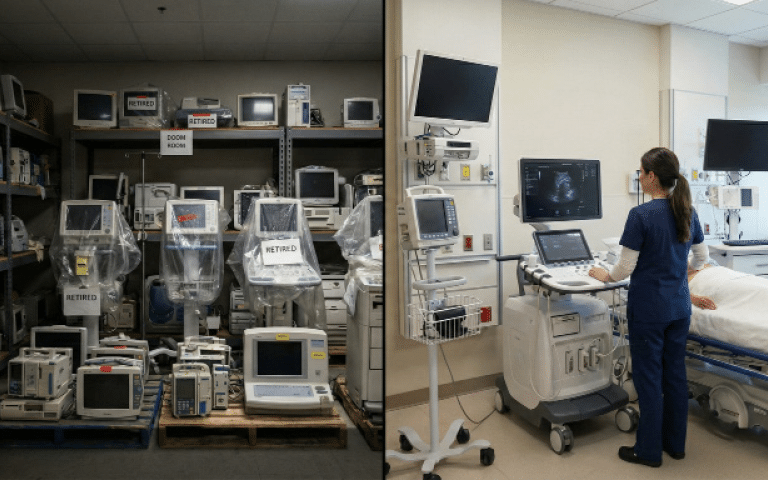
Lynskey: The biggest mistake is treating equipment retirement like an afterthought instead of a clinical and financial decision. We see hospitals park devices in hallways, closets or “doom rooms” for months waiting for someone to deal with it. That creates compliance risk, lost resale value and inventory blind spots. Another common miss is skipping proper documentation and chain-of-custody tracking. If you can’t prove what happened to a device, that’s a problem. And finally, too many organizations default to scrapping equipment that still has usable life or parts value. That’s literally throwing money away.
Arcadi: They often choose a lower cost service provider during the life of the equipment’s use, which can have a large negative impact on the value of the equipment during trade-in or sale. It also shortens the useful life they could get out of that asset
Thomason: One of the biggest mistakes is equating “no longer right for us” with “no longer valuable.” In U.S. health systems, equipment is often retired because of standardization initiatives, technology upgrades or service contract changes – not because it’s unsafe or unusable. But globally, the need is staggering. The World Health Organization estimates that nearly half of the world’s population lacks access to essential health services. In many low-resource settings, clinicians are working without reliable imaging, anesthesia or even basic monitoring equipment. So, what may be a prior-generation ultrasound in Phoenix or Chicago can be the first ultrasound in a regional hospital in Ghana or Nepal. Another mistake is looking only at secondary market value. Financial resale price doesn’t capture patient impact. When we talk about disposition, we should be weighing both economic return and healthcare return.
Q: WHAT STEPS MUST BE TAKEN TO PROTECT PATIENTS AND MEET HIPAA REQUIREMENTS WHEN IT COMES TO EQUIPMENT DISPOSITION AND RECYCLING?
Lynskey: It starts with data. Anything with memory, storage or network connectivity needs certified data wiping or physical destruction before it ever leaves the building. That includes monitors, imaging accessories, telemetry, infusion systems, and even certain beds and specialty devices. We always work directly with each facility’s IT and security teams to ensure we are following their HIPAA requirements and internal e-waste policies, not just generic best practices. From there, it’s about documented chain-of-custody, serialized tracking and responsible environmental handling for batteries, fluids and electronic waste. At HERO, we treat disposition like an extension of the HTM program, not a junk pickup. Patient safety, cybersecurity and sustainability all live in the same lane here.
Thomason: Patient privacy is non-negotiable. Any device that stores protected health information must be properly sanitized in compliance with HIPAA. That means secure data wiping and removal or destruction of hard drives where necessary. At the same time, we have to be thoughtful. Data security shouldn’t automatically mean physical destruction of equipment that could safely serve patients. Due diligence is essential, and donation or disposition partners need to have processes in place to ensure safe transition of equipment and transparency about where equipment ultimately goes.
Q: WHAT FACTORS SHOULD HEALTHCARE ORGANIZATIONS CONSIDER FIRST WHEN DECIDING WHETHER TO REDEPLOY, RESELL, RECYCLE OR DISPOSE OF MEDICAL EQUIPMENT?
Lynskey: The first question should always be: Does this asset still have clinical or operational value? Redeployment within the system is often the fastest ROI. Next is condition, serviceability, parts availability and regulatory status. After that, market demand and resale potential come into play. If the device has no redeployment or resale value, then recycling and responsible disposal are the right move. The key is having a structured decision framework instead of making emotional or convenience-based calls.
Arcadi: Choose a trusted equipment partner and stick with them on the front end of an equipment purchase, during the useful life of the asset and when trading it in for a newer piece of equipment at the end of its useful life.
Thomason: I would start with alignment. Healthcare organizations exist to improve health outcomes. Equipment donation is an opportunity to extend that purpose beyond your walls. Next, take a realistic look at net financial impact. What are the actual net proceeds after broker fees, logistics, refurbishment, staff time and storage costs? In many cases, resale yields less than expected once all costs are accounted for. Donation can provide tax-deductible value while also advancing community benefit goals and ESG commitments. It also eliminates warehousing costs and frees up space quickly when working with the right nonprofit partner. Don’t forget about operational efficiency. Does your disposition partner provide pickup, documentation and streamlined logistics that quickly free up valuable space and staff resources? And finally, consider supportability. Is the equipment serviceable? Are parts available? Responsible nonprofit partners assess these factors before accepting your donation to ensure equipment strengthens health systems rather than burdens them. A fundamental guideline – would you feel comfortable using this equipment on someone you love.
Q: WHAT OPPORTUNITIES EXIST TO RECOVER VALUE FROM RETIRED OR SURPLUS MEDICAL EQUIPMENT?
Lynskey: There’s more value sitting in hospital back rooms than most people realize. Resale of complete systems, harvesting high-demand parts, redeploying accessories and refurbishing select assets can all drive real dollars back into capital budgets. Clinical assets like beds, stretchers and specialty patient care equipment often represent some of the highest return opportunities when managed correctly. When disposition is done strategically, it becomes a revenue recovery program instead of a cost center.
Arcadi: Properly maintain it during its life and knowing the sweet spot of the asset’s trade-in value a few years ahead of time.
Thomason: There are three kinds of value to think about. First is humanitarian value. The Lancet Commission on Global Surgery reported that five billion people lack access to safe, affordable surgical and anesthesia care. Equipment plays a central role in closing that gap. Reliable operating tables, lights, anesthesia machines – these aren’t luxuries; they’re prerequisites for safe care. Second is environmental value. Extending the life cycle of medical equipment reduces waste and aligns with circular economy principles. Healthcare generates significant surplus globally, and responsible reuse keeps usable technology out of landfills. For us, sustainability is a beautiful by-product of what we do, however our focus is building stronger healthcare systems. Third is financial and reputational value. Donation can generate tax benefits and demonstrates to stakeholders – from employees to patients to boards – that your organization is committed to health equity and responsible stewardship. Value recovery is bigger than resale dollars.
Q: WHAT ELSE SHOULD TECHNATION READERS KNOW ABOUT EQUIPMENT DISPOSITION AND RECYCLING?
Lynskey: This is not just about getting rid of stuff. It’s about protecting patients, safeguarding data, supporting sustainability goals and being good stewards of hospital resources. When HTM teams own this process or partner with the right experts, it becomes a powerful extension of the department’s value. At HERO, we believe disposition should be transparent, documented, compliant and financially smart. If it feels messy, unclear or risky, that’s a sign the process needs an upgrade.
Arcadi: Learning the various “use & hold” strategies for buying, using, servicing and capitalizing on the asset at the end of life. You can go shorter term life and maintain it less, or you can invest in proper service and extend the life of the asset for 5 or more years
Thomason: Discarding equipment without evaluating its potential impact should truly be the last step. Well placed donations are done responsibly. Equipment should be tested, matched to validated needs, and placed with facilities that have the capacity to use and maintain it. When done well, equipment donation strengthens health systems and expands access to care. At Project C.U.R.E., our model is built around needs assessments, biomedical testing and careful placement – because our goal isn’t simply to move equipment. It’s to ensure healthcare for people who otherwise might go without it. Disposition isn’t just an operational decision. It’s a strategic one – with implications for global health, sustainability and your organization’s legacy.
For more information about Project C.U.R.E. visit projectcure.org.
