

 At the 2017 South by Southwest Conference in Austin, Texas, a panel discussion entitled “The Sound of Robots” was held to “highlight how the voice of robots could influence the interaction between human and robots.” This panel, part of the conference’s “Intelligent Future” track, discussed how voice influences interaction between humans and robots. Does the way a robot sounds portray its personality? Should your robot have its own personality selected by you? If humans are mean to robots, should the robots respond in kind? Should they always be listening to our conversations – particularly intimate ones?
At the 2017 South by Southwest Conference in Austin, Texas, a panel discussion entitled “The Sound of Robots” was held to “highlight how the voice of robots could influence the interaction between human and robots.” This panel, part of the conference’s “Intelligent Future” track, discussed how voice influences interaction between humans and robots. Does the way a robot sounds portray its personality? Should your robot have its own personality selected by you? If humans are mean to robots, should the robots respond in kind? Should they always be listening to our conversations – particularly intimate ones?
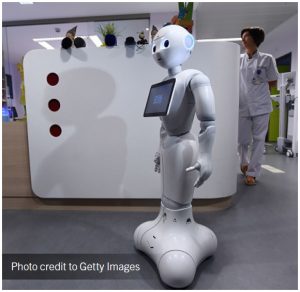
As humanoid robots are introduced into health care facilities, these are all important considerations for health care leaders. In fact, ECRI Institute highlighted “Pepper the Emotional Robot” in its 2017 C-Suite Technologies to Watch monograph. Pepper is touted as the world’s first humanoid robot which interprets human body language, reads emotions, and responds accordingly. In 2016, two Belgian hospitals introduced Pepper in their reception areas to support reception staff by meeting and greeting visitors, answer questions in any of 19 languages, collect information, and escort people as needed to physician offices or other areas. The robot body is about four feet tall, has a head filled with sensors, eyes with colored lights, a tablet device integrated into the chest area, and arms that can move in 17 directions. The light color of the eyes changes according to the perceived mood of the surrounding people. Pepper has a combination of 2-D and 3-D cameras to help it process images with shape-recognition software to identify objects, faces, and emotional states. With all this embedded technology, Pepper can recognize faces, speak, hear someone speaking, move autonomously, and engage in conversation.
Pepper is just one example of artificial intelligence and robots gaining a foothold in patient care. While it is an off-the-shelf robot, its programming had to be developed extensively for its range of tasks. With the baby boomer generation living longer independently, or living longer in their own homes with chronic diseases, there is a growing need for assistive technologies like Pepper. Intelligent robots integrated with Smart Home sensors may be a necessary link in the continuum of care; they can be used to assist the older adult – and their caregivers – with tasks related to independent living and cognitive assistance. However, how these are deployed and subsequently supported create an entire new set of challenges for health care providers.
First, these robots probably need a dependable internet service as well as integration with other monitoring/sensing technologies. If we think that wireless coverage in a hospital basement or elevators is a challenge, wait until dealing with the challenges of outdated routers in people’s residences. It’s one thing when a social worker visits a home to look for tripping risks such as area rugs; it’s another skill set entirely to wire a residence with a monitoring system that uses cameras and speakers and then conducting home Internet bandwidth assessments. How many clinical engineering or information technology departments have the extra personnel to take on this task? Or, is this something that the local visiting nursing association will handle?
Second, many of these robots are likely to use the cloud to send and store information. This creates security issues from both a patient privacy perspective and a protected health information (PHI) perspective. As developments in point-of-care technology and medical devices for home use are made, these robots may evolve into more than just companions and actually “provide” care for a patient with a chronic or rehabilitative condition. Many of us are already hesitant when it comes to a friend placing technology in our home setting; the acceptance of a robot may depend on its “humanity” as much as its security designs.
In a hospital setting these issues may be a bit easier to handle, and the management of the fleet of humanoid robots may be overseen by Clinical Engineering, IT Application Support, Environmental Services – or an entirely new service function. In the acute care setting, humanoid robots might develop to support other tasks like patient watching or routine vital signs monitoring. However, this may not be the case too much longer. A recent New York Times Magazine article (February 26, 2017) on the new working class in America suggested that “The most important frontier for robots is not the work they take from humans but the work they do with humans.” The article explored how new software and operating instructions could enable robots to do many of the tasks required of waiters, maids and hospital workers. On another robot related front, there are collaborative robots, which are focused on specific tasks instead of an entire job’s skill sets, which are poised to be implemented soon. These ultra-focused robots will do specific repetitive tasks like take a temperature or a blood pressure reading.
Whether humanoid or task-specific robots gain staff acceptance, let alone patient acceptance, has yet to be determined. Pro-active hospital leaders should be assessing where robots may play a role in care settings. Does it make sense to have a fleet of robots as greeters at each and every access point to the hospital? Which department will be responsible for operational management of these robots, and what skill set will personnel in this department need to do so? Can a collaborative robot be developed to decontaminate surgical instruments, thus eliminating a personnel hazard exposure risk? Currently, chemistry and hematology lines in the clinical laboratory are largely automated, but can robots somehow be used there? What will be the next collaborative task that is undertaken? And most importantly, will the robots look like Rosie from the “Jetsons” or will it be a more menacing and pervasive presence like HAL 9000 from Stanley Kubrick’s “2001: A Space Odyssey”?
ECRI’s Applied Solutions Group can provide customized consulting services to health care organizations interested in incorporating Pepper and other health care technologies into their suite of services. Learn more at www.ecri.org/appliedsolutions.
This article is excerpted from ECRI Institute’s 2017 Top 10 Hospital C-Suite Watch List. To download the full report, visit www.ecri.org/2017watchlist. For more information on ECRI Institute’s evidence-based health technology assessment or consulting services, contact communications@ecri.org, or call (610) 825-6000, ext. 5889.
