

![]()
In June 2024, ECRI convened a panel discussion to share best practices for optimizing telemetry monitoring implementations to reduce alarm fatigue and improve patient safety. Interested readers can view the full webcast at the URL listed below.
Telemetry monitors are patient-worn devices that allow the patient’s heart rate, heart rhythm and other physiologic conditions to be assessed without restricting the patient to a bed. These devices allow cardiac patients to move around the facility – if they are well enough to do so – while still being monitored. However, inappropriate deployment protocols, alarm settings, or notification processes can prevent staff from learning about potentially life-threatening changes in the patient’s condition or can lead to alarm fatigue. The result can be missed alarms and potentially severe consequences for the patient.
Panelists who participated in ECRI’s June 5, 2024, webcast emphasized that a safe, effective telemetry monitoring program requires a good alarm management strategy. Following are some of their key recommendations.
1. Avoid Telemetry Overuse
Early in the program, Priyanka Shah – a principal project engineer in ECRI’s Device Safety group – presented one of ECRI’s key recommendations for reducing nuisance alarms and alarm fatigue: Do not use telemetry monitoring on patients who do not require that level of monitoring.
Ms. Shah used the example of ECG “leads off” alarms to explain the recommendation. Leads-off alarms are a common occurrence with telemetry monitoring. They warn care providers that the telemetry monitor has lost contact with the patient, often because an ECG lead has become detached from, or is in poor contact with, the patient’s skin. In some cases, the alarm could be a precursor notification for a lethal arrhythmia. For patients with cardiac conditions, leads-off alarms must be addressed immediately, since they indicate that the patient is not being monitored (or could be experiencing a potentially lethal arrhythmia).
Now consider a scenario in which all patients in a care area are placed on a telemetry pack, even patients who are not at risk of a cardiac event. For that latter group of patients, a leads-off alarm would be less urgent because the patient’s condition may be non-cardiac or of a lower acuity, such that ECG monitoring is not required. Thus, an interruption in ECG monitoring is unlikely to be as clinically significant as it would be for cardiac patients.
Nevertheless, leads-off conditions will occasionally occur among all monitored patients, and alarms will activate. That means staff will be faced with determining which leads-off alarms are critical, and which are low-priority. That’s a recipe for alarm fatigue and missed alarms.
A more effective strategy is to use telemetry monitoring only on patients who are determined to be at risk. That will reduce the overall number of alarms that activate, as well as minimize confusion about the priority level of leads-off alarms. Similarly, telemetry monitoring should continue only as long as the patient’s condition requires it. Organizations should follow AHA guidelines and define clear criteria for initiating – and discontinuing – telemetry monitoring.
2. Consider the ‘Human Element’ – What Do Staff Members Need?
Rosemary Wurster, DNP, RN, NEA-BC – a senior vice president and chief nurse executive at Bayhealth – provided the clinician’s and administrator’s perspective. One of her key recommendations is that facilities should always consider the “human element” when implementing and evaluating technology. “As an organizational leader, it’s very important for me to think about how my greatest resource – my people – will be interacting with the technology. How can we create a work environment that helps them do their jobs effectively?”
Panelists discussed the example of telemetry implementations that use a monitor watcher room, sometimes referred to as a “war room.” In such setups, it’s important to review every detail – things like: how the room is configured, who is performing the monitoring watching function, what their working conditions are like, how they receive information about the patient, and how they communicate alarm information to care providers at the bedside. Other questions to think about include: Is the working environment both functional and comfortable? Are restrooms easily accessible? Are staff given sufficient breaks, so that they can rest physically and mentally? And is sufficient coverage provided during those times?
Additionally, Wurster stressed the value of recognizing that monitor watchers are part of the care team. When savvy staff in the monitoring room observe an issue with a patient and communicate it to the care providers, they get invested in that patient’s care. Teams should close the loop with those monitor watchers, describing how the situation was resolved so they can recognize the full value of their contribution.
3. Assess Practices on All Shifts – Days, Nights, and Weekends
Best practices for assessing an organization’s alarm management strategies were described by Marc Schlessinger, a senior consultant and investigator for ECRI’s Healthcare Incident Investigation & Technology Consulting program.
ECRI recommends activities like those that it performs during its proactive assessments of monitoring utilization and alarm management for interested health care organizations. These assessments include three main components: (1) An evaluation of the facility’s policies and procedures. (2) A review of recent incidents and near misses related to monitoring that have occurred at the facility. And (3) site visits to the care areas where telemetry is used, so that evaluators can assess the physical layout, observe practices and interview staff.
To get the full picture, Schlessinger emphasized the need to assess practices during all shifts – days, nights and weekends. “Anybody who has ever worked at a hospital knows that what happens at 9 p.m. may not be the same thing that happens at 4 p.m. It’s important to get a 24-hour perspective of what’s happening.”
4. Have an Active Alarm Management Committee
All panelists agreed that alarm management needs to be an ongoing effort. “Leadership has the responsibility to be continuously evaluating the effectiveness of the organization’s processes,” stressed Wurster. “Health care changes quickly. Technology changes quickly. We’re in an environment with significant staff turnover. All those factors contribute to the need to continuously evaluate how things are being done, and whether current processes are meeting the organization’s patient care goals.”
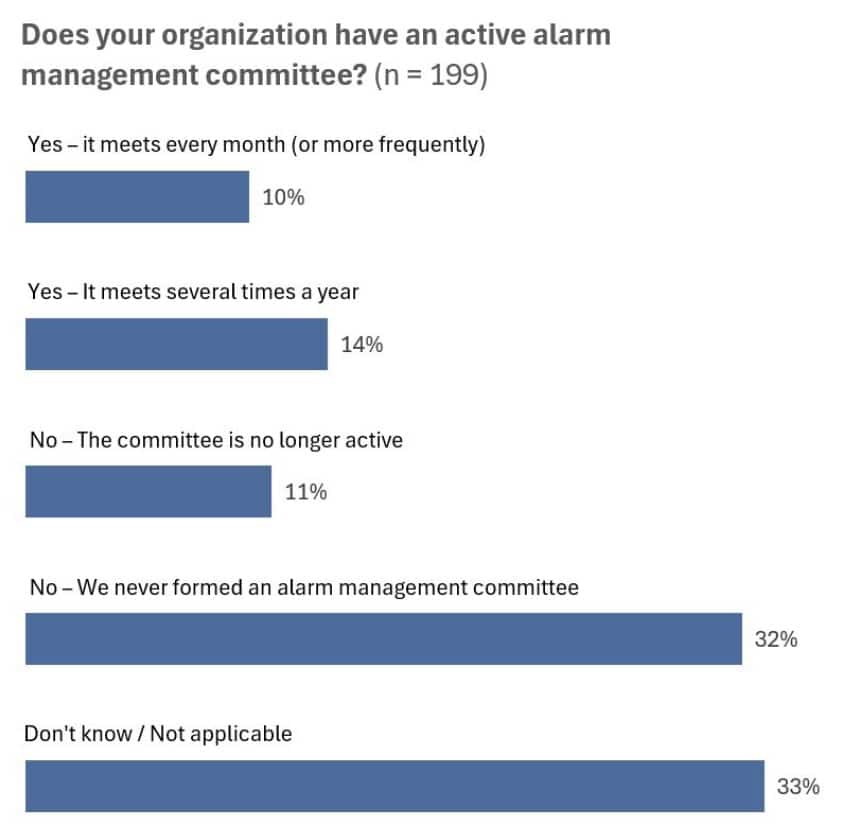
Managing that ongoing effort would be the role of an organization’s multidisciplinary alarm management committee. Unfortunately, many facilities lack such a committee: Almost half of the 200 respondents to a poll conducted during ECRI’s webcast indicated that their facilities do not currently have an active alarm management committee.
To Learn More . . .
To view the full webcast, visit: https://ly.ecri.org/LabWebcast2024_TelemetryAlarmManagement.
For more information about ECRI’s Monitoring Utilization & Alarm Management proactive assessment services, email TechConsulting@ecri.org or contact ECRI by telephone at (610) 825-6000, ext. 5891.
