

![]()
By Barbara G. Malanga, BSEE
Delayed awareness and a lack of reporting can have profound effects on the healthcare incident management and investigation process. For example, if no one brings an incident to the attention of the Risk Manager or other appropriate person, it can happen again before the underlying causes are identified and addressed. Creating a culture in your facilities where incidents are immediately reported so that the appropriate early steps can be taken is paramount to patient safety and investigational success.
One of ECRI’s member hospitals asked us to investigate an incident involving an Alaris infusion system after a nurse reported suspected free-flow of medication from a large volume pump (LVP).
The hospital sent ECRI an Alaris Patient Control Unit (PCU) with 3 Large Volume Pumps (LVPs) attached to it for inspection and testing.
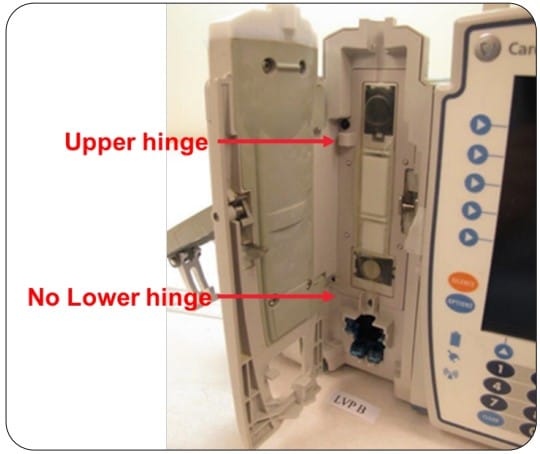
Visual inspection immediately identified the problem. The inner platen door on the suspect LVP was missing. The inner platen door is responsible for compressing the pump segment tubing to control flow as the pump cycles, and prevent gravity flow. We also noticed that the lower platen door hinge and its retention rivet were absent, and a piece of the Flo-Stop receptacle was broken off and absent.
ECRI concluded that the platen door was most likely displaced from the LVP by a forceful impact when the LVP outer door was open. This results in the pump allowing gravity flow through a properly installed Alaris IV set even if the pump is stopped, not yet programmed, or turned off.
We proceeded with testing to see if there was an alarm produced to warn the user that there was something wrong. The PCU was turned on successfully and immediately produced a “Check IV Set” Alarm.
Analysis of the pump’s logs showed that at the time of the reported free-flow the IV set was installed in the incident pump and the user interacted with the pump for almost 10 minutes during which time multiple “Check IV Set” alarms occurred. These alarms were silenced multiple times as the user probably tried to troubleshoot the problem. During that time the patient received by gravity delivery ~50 mL/minute of the drug to be infused.
Further log review indicated that the pump had been in service without its platen door for approximately one month prior to the reported incident. Over that time many attempts were made to administer infusions with it. It is likely that multiple incidents of uncontrolled flow occurred before the unresolvable “Check IV Set” Alarms caused users to obtain and use a different LVP.
ECRI sees this problem often – users use workarounds or move on to another pump and do not report problem devices.
AWARENESS
Incident awareness in the health care setting begins with the specific knowledge of an injury or its reasonable likelihood. Incident awareness most often starts with the clinical staff. While providing care they may recognize that something unexpected has occurred. For example, while caring for their patient the staff may recognize that an unexpected complication or injury has occurred; or they realize that there could have been a “near miss” or “close call.”
Medical devices are in many cases integral to the delivery of health care. Ignoring a device that makes an unexpected noise, repeatedly alarms, or is noticeably broken can result in a health care incident – an unexpected injury, complication or death. Staff should be trained and encouraged to be on the look-out for unexpected device performance and report it when it happens.
REPORTING
Reporting medical-device-related problems is crucial for keeping patients and staff safe. Unfortunately, problems aren’t always reported through appropriate channels, if at all. The reasons for this can vary:
- Device users may be focused on patient care and unable to interrupt a time-sensitive task to submit a report.
- They may be unfamiliar with the method for reporting.
- They may see little benefit to reporting, particularly if no harm was observed.
- They may intend to report the problem but fail to, due to busyness.
- They may fear disciplinary action or other personal consequences.
As a result, broken, malfunctioning, poorly manufactured or poorly designed devices may remain in use.
Attempting to use faulty or suspect devices can, at the very least, waste clinician time as users try to effect workarounds or to quickly locate replacement equipment. More significantly, continuing to use such equipment can lead to patient harm.
In contrast, when problems are reported as soon as they are noticed, they can often be remedied before patient care is affected. To achieve this goal, health care organizations need to identify and eliminate barriers to reporting. Measures that can be taken include:
Make reporting easy!
- The reporting process should be as easy as possible to minimize disruptions to patient care tasks.
- Create a well-defined reporting process that is consistent across departments
- Consider incorporating the ability to report adverse events into the clinical workflow, if possible
Build a culture of safety (to encourage reporting).
- Every effort should be made to create a culture where incidents are immediately reported because delayed awareness can have profound effects. For example, accessories may be discarded, hindering the subsequent investigation. If equipment that should have been sequestered continues to be used it can result in loss of stored incident information, or the problem can happen again perhaps with a more severe outcome.
- Make reporting safe by establishing an internal reporting mechanism that encourages open and forthright communication without fear of reprisal. Consider allowing reporting to be confidential and optionally anonymous.
Educate staff about how to identify potential hazards.
- Educate staff on what types of occurrences should be reported internally and to whom, providing examples of situations in which reporting is needed, such as: deaths, injuries, near-misses, repeated device failures, hazardous practices, or staff impairment.
- Training can help staff understand the importance of awareness and reporting as well as regulatory and accreditation reporting requirements.
Provide feedback to keep staff informed about the status of a report.
- Acknowledge the reporter and assure them that their report will be acted on
- Promote “wins” – that is, instances in which a report prevented significant harm or led to meaningful improvements.
- Provide support while you investigate what happened, recognizing that caregivers may be victims also.
PREVENTING RECURRANCE
“The goal of any healthcare incident investigation is to determine what happened and take the necessary steps to prevent recurrence,” explains Scott Lucas, ECRI’s vice president of device safety.
Following the investigation described above, ECRI investigators visited the reporting hospital and performed a Proactive Assessment related to infusion pump management. They reviewed the health system’s practices and procedures related to the overall infusion pump fleet and infusion pump incident management.
Specifically, ECRI gathered information from relevant staff to identify common technical problem areas and assess cleaning methods, pump distribution, available storage, and pump incident reporting and sequestration practices.
Opportunities for improvement were identified. With regards to incident reporting and sequestration, ECRI recommended the hospital utilize a standardized tagging system to clearly identify those pumps that should not be used, needed to be evaluated, or needed repair. ECRI also recommended that procedures be put in place and staff training on pump incident reporting and proper equipment sequestration to ensure that when a problem is identified that all associated pump modules and incident consumables are sequestered, allowing follow-up assessment and testing of the entire system.
For Bruce Hansel, chief scientist and principal investigator for ECRI, this case emphasizes the need to have policies and procedures for removing “problem” or suspect devices from service. He advises “When in doubt, tag it out!”
TO LEARN MORE …
Awareness and reporting are the first two steps in ECRI’s IMI Plan. The IMI Plan includes 7 points to consider in the management and investigation of healthcare incidents with a focus on helping to improve the process and prevent missteps. Technology managers and other healthcare professionals can learn more about the IMI Plan through ECRI’s Healthcare Incident Management and Investigation eLearning course.
To learn more about ECRI’s Proactive Assessments or to inquire about a third-party independent incident investigation, click here. Contact ECRI by telephone at (610) 825-6000 ext. 5891, or by email at client services@ecri.org.
Barbara G. Malanga, BSEE, is the director, preventive solutions and device safety operations, ECRI.
