

 ECRI Institute’s Health Devices engineering team recently completed an evaluation of three automated whole-breast ultrasound scanners. This excerpt from the published study describes some of the purchasing considerations that the group identified during its testing.
ECRI Institute’s Health Devices engineering team recently completed an evaluation of three automated whole-breast ultrasound scanners. This excerpt from the published study describes some of the purchasing considerations that the group identified during its testing.
Technology Overview
Automated whole-breast ultrasound (AWBUS) scanners were developed primarily to address two concerns: (1) the limitation of screening mammography to detect breast cancers in women who have dense breast tissue and (2) the user-dependent and time-consuming nature of conventional handheld ultrasound of the breast.
The limitation of screening mammography has prompted more than 25 U.S. states to enact what are called “breast density laws.” (Similar laws are being considered in several additional states.) Although the requirements vary from state to state, breast density laws typically require that women who have dense breast tissue, as identified with mammography, be notified by their physicians about the limitations of mammography to detect breast cancer in dense breasts. The laws further specify that these patients be offered options in their care, including receiving additional imaging exams. (For more details, see: http://www.diagnosticimaging.com/breast-imaging/breast-density-notification-laws-state-interactive-map.)
Ultrasound is one of several imaging modalities that may be used as a supplement to mammography to improve the overall efficacy of breast imaging for patients who have dense breasts. Tomosynthesis and magnetic resonance imaging are other modalities that may be used.
The breast density laws, along with the commercial availability of AWBUS models from several vendors, have fueled interest in AWBUS as a supplement to mammography. AWBUS examinations are typically performed after a screening mammogram; the two modalities provide complementary data.
AWBUS scanners represent a technological advancement over conventional handheld breast ultrasound in that they automate the acquisition of ultrasound images of the breast and facilitate review of images for formal interpretation by a physician. Specific advantages compared with handheld ultrasound include the following:
- AWBUS scanners improve reproducibility and reduce interobserver variation.
- Exam performance and results are less operator-dependent than with handheld ultrasound.
- Data acquisition is more time-efficient and is separate from diagnostic interpretation, thereby enhancing workflow.
- AWBUS scanners provide a large field of view that enhances the ability to localize pathology in relation to anatomical landmarks, such as the nipple.
Form and Function
Ultrasound imaging systems transmit high-frequency sound waves into the patient and receive echoes that result from the interaction of the sound waves with body tissues. These systems use a transducer to transmit and receive the ultrasound signals; these signals are then used to create images on a video display.
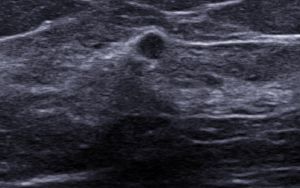
AWBUS systems automate the acquisition of “B-mode” ultrasound images of the breast – these images depict anatomical structures in grayscale. Some AWBUS scanners have additional imaging capabilities, such as Doppler modes that are used to assess blood flow and improve characterization of breast disease.
AWBUS systems are currently available in two forms:
- Articulated-arm-style scanners use a transducer attached to an articulated arm that can be positioned over the patient. The patient lies on her back on a table, and the transducer is placed in contact with the patient’s breast. Once activated, the transducer mechanically sweeps across a region to acquire a series of 2-D ultrasound images of the breast.
- Table-style scanners use a dedicated table that houses a transducer within a recessed portion of the table. The patient lies face-down on the table with one breast positioned over the transducer. Once activated, the transducer rotates 360° to acquire a series of radial 2-D images.
 With both designs, the acquired 2-D images are sent in standard format to a workstation, where they are compiled to form a volume data set that is used for review. AWBUS systems use specialized software on the workstation to improve diagnostic interpretation and facilitate time-efficient workflow.
With both designs, the acquired 2-D images are sent in standard format to a workstation, where they are compiled to form a volume data set that is used for review. AWBUS systems use specialized software on the workstation to improve diagnostic interpretation and facilitate time-efficient workflow.
Comparing Systems
ECRI Institute recommends that healthcare organizations consider factors such as the following when selecting an AWBUS system.
Intended Applications
Some AWBUS devices are indicated for screening and diagnostic imaging applications, while others are indicated only for diagnostic imaging applications.
Configuration: Dedicated Device versus Add-on to a Conventional Scanner
Some AWBUS systems are dedicated devices that can be used only for automated acquisition of B-mode breast ultrasound images. An additional ultrasound scanner is required if the clinician wants to, for example, use ultrasound to evaluate the patient’s axilla for lymph node disease, acquire Doppler data, or perform an ultrasound-guided biopsy.
Alternatively, some AWBUS devices connect to a conventional ultrasound scanner. When not being used for AWBUS exams, the conventional ultrasound scanner equipped with handheld transducers can be used:
- For non-breast applications (e.g., obstetrical ultrasound exams)
- To better characterize breast masses detected with AWBUS by using color Doppler imaging (CDI) to assess the vascularity of the mass or by using elastography to assess the relative stiffness of the mass
- For ultrasound-guided breast biopsies
If a facility already owns a conventional scanner that is compatible with an AWBUS component, this could represent a cost saving. Note, however, that if the conventional scanner is used to acquire additional data – such as CDI to assess blood flow in a mass, or elastography to assess tissue stiffness – operators must possess the skills needed to effectively use these additional modes.
Form: Articulated-Arm-Style versus Table-Style Scanners
Articulated-arm-style systems are easier to move and may require less physical space than table-style scanners. With this type of scanner, however, operators must have the skills to determine whether additional data acquisitions are required to ensure a thorough exam of the patient, and if so, how many.
Some patients may feel more comfortable being examined on a table-style AWBUS scanner because their breasts are not exposed as much and require less manual manipulation compared to an articulated-arm-style scanner.
Performance: What ECRI Institute Looks For
When testing the performance of AWBUS systems, ECRI Institute uses industry-standard quality assurance tests and a custom-designed breast-tissue-mimicking phantom to objectively determine:
- Spatial and contrast resolution
- Image uniformity and tissue penetration
- Accuracy of distance measurements and calculations
The organization also looks at safety concerns, answering questions such as: What ergonomic features are present, and does the system have any components that could cause injury to users or patients?
To examine the impact of each system on workflow, the group considers, for example:
- Is the user interface easy to operate?
- How many data acquisitions are required on an average-size patient?
- How much time is required to perform a bilateral examination, including patient preparation, positioning, data acquisition, and data transfer?
- Are there any patient-related limitations (e.g., breast size, the patient’s physique) that could affect use of the device?
- What are the hardware and software requirements?
- What image interpretation software features and tools are available?
The organization also assesses:
- Breast compression features for how they affect patient comfort
- The ability to integrate the device into a facility’s existing health IT infrastructure
- Inspection and preventive maintenance requirements
- The total cost of ownership
In its recent evaluation, ECRI Institute found that all three of the tested models offer acceptable performance. Differentiating factors include the intended applications, configuration, and form, as described above, as well as some features affecting workflow, the user experience, and total cost of ownership.
This article is excerpted from ECRI Institute’s “Evaluation Background: Automated Whole-Breast Ultrasound Scanners,” Health Devices 2016 March 23. The complete article – including model-specific test results and product ratings, along with additional guidance for purchasing and using this technology – is available to members of ECRI Institute’s Health Devices System and associated programs; learn more at www.ecri.org/components/HDS.
